“Hi doctor X! You’ve got free air in your abdomen.” Doctor X is a pediatrician, rotund and florid. He is rather excitable and has a vivid imagination. You often expect him to have a cerebral hemorrhage during a conversation (blow a gasket). He is a great story teller with artistic tendencies, and has good rapport with children and their parents. A bit unorthodox perhaps, but never boring. “I can sell this darling on the internet for you,” he said once when some parents were complaining about their son’s stomach. Well, the doctor had been seen by the surgeon on call, because of an abdominal pain, who had promptly ordered a CT scan because of his abdominal pain. After the examination he&the patient somehow got through the cracks and just went home. The surgeon on call came across the CT later in the day and there it was — free air in the abdominal cavity (which means there is a hole in a bowel somewhere). The surgeon immediately contacted Doctor X and ordered him to come post haste to the hospital. Understandably Doctor X got really scared, and with his imagination racing, thought his days were numbered. He was expected to return within the hour, but time dragged on, and finally he shows up obviously freshly shaven and sporting a new haircut! “Where the hell have you been?” was the first question. “I am certain that I am not going to make it,” came the retort — “that´s why I went to have a haircut and a shave.” Now the surgeon is incredulous “we fix this all the time you idiot” (is that how you talk to a pediatrician?). “No, I am a goner,” he continues, “to be on the safe side I also had my portrait taken by a professional photographer – in black and white for effect. Something for my family to remember me by.”
His treatment was uneventful, and he recovered. Since that time, he has a new found respect for surgeons and thinks we are miracle workers, nothing less. Doctors are a very difficult group to deal with as patients. Especially those who are cynical and meddle in their treatment plans. The only group that is worse is probably the clergy. “It is all in His hand” type of reasoning can get you to a boiling point. “Perhaps He put us here to take care of you” reasoning does not seem to enter their minds.

Neskirkja í Aðaldal
At the end of my training I used my vacation to do locum work at my first surgical department. I was a newly minted surgeon (licensed and all), and it was common for new specialists to do locum work in Iceland instead of taking a vacation. The family got to go home to all the relatives, and we got some brownie points for relieving the staff doctors. It was a bit like a dress rehearsal, where we could show just how good we were and also get a feel for working there for the future.
The atmosphere at the surgical department was jovial, and the morale good. The rhythm of the day was to present new patients at the morning meeting. The emergency patients were discussed, and any problems incurring during the last 24 hours were recounted. I had been on call, and we had admitted an old lady with a distended abdomen in the morning hours. She was emancipated and in dire straits, and the bowels were obstructed. What to do? Well, first off you discuss that with your patient. She understood that an operation was very risky, but by doing nothing she was going to die. She still enjoyed life she told me, and we decided on an operation as our only option. The staff surgeons were very negative about this endeavor. One of them of the “It is none of your damn business” fame (see my blog, https://everyjonahhasawhale.com/?p=1811) thought me mad. “Are you going to operate on that mummy?” He went on and on about it. Then there were the anesthetists! “The electrolytes are terrible, the kidney function impaired and my god that heart.” Well, I honestly love anesthetists and I understand their plight. First, they have to anesthetize such a person, and then they have to deal with the surgeon – at the same time. So, the discussion with the anesthetists on the merits of such an operation, and the risks involved could be interesting. My central argument was always simple. The primary disease process causing all those abnormalities in the electrolytes, etc. was perhaps, and quite likely something that could be reversed. Our philosophy is, if the primary process can be fixed, the secondary problems have a chance of getting better. So, the patient will only survive the operation that fixes the primary problem. We must be very focused on that, and actually try to simplify things (some might call it tunnel vision). If you do not do that you will become mired in minutiae, and you can not do anything at all because it is all so terrible and rapidly getting worse. My arguments carried the day, and the anesthetists got the old lady ready for an operation. I was about to open her abdomen when the door of the operating room banged open, and the surgeon with his walrus mustache barged in.
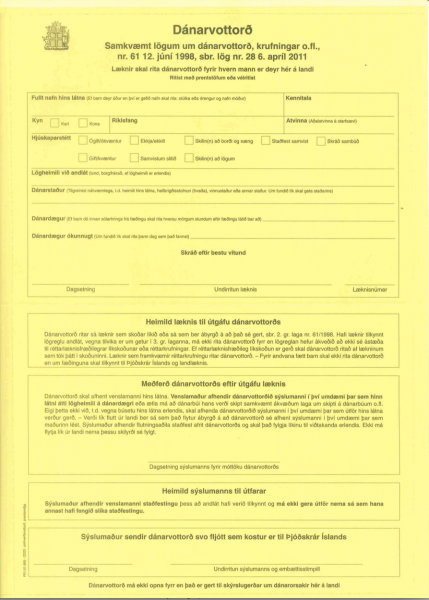
Dánarvottorð – Death certificate
He was in fine spirits and was holding a pen in one hand and a death certificate in the other hand (those forms were the only ones we used on yellow paper.) Then he bellows – “When you start cutting – I will start writing!” He really was a lovable scoundrel.
There you go – what an auspicious start to an operation. By that time, I was getting to know him and I suspected that he was only “weighing my cojones,” so I did not get too rattled. All this black humor is a coping mechanism in a stressful environment. The operation was easy, and I found the suspected incarcerated femoral hernia, which was easy to fix. This lady recovered nicely and was duly discharged.
I sit here alone on the banks of the river
The lonesome wind blows and water runs high
I can hear a voice call from out there in the darkness
But I sit here alone too lonesome to cry
The Lonesome River – Bob Dylan
For doctors the river is constantly there. Our lives are lived on the banks of the river. Sometimes our toil is to prevent early departures and sometimes it is to help people to navigate across. We might as well fish it while we are at it!